Note: This opinion piece reflects my personal views and not those of any group with which I am affiliated. A PDF version is available here.
For reasons I don’t understand, the American Psychologist, the flagship journal of the American Psychological Association (APA), has published another article that appears to misrepresent antisemitism and its prevalence within the mental health professions (this isn’t the first time). The authors who wrote “Is It Really That Bad? Antisemitic Experiences Among Jewish Mental Health Professionals” — Micah Brosbe, Caroline Kaufman, Elizabeth Getzoff Testa, Karen Dimentstein, Danielle Guttman-Lapin, and Tali Rasooli — claim that their online survey revealed widespread antisemitism in these work settings. But based on my review of the article, I don’t believe their findings demonstrate anything of the sort. And I think it’s important to highlight this, because there are individuals and groups that nevertheless will promote and cite this article to support their political agenda. So, let’s take a closer look.
Non-Representative, Biased Sampling
The most fundamental reason to discount this research is that it’s based only on responses from a narrowly selected group of participants. Although the authors state that they collected data “from a wide range of Jewish mental health professionals,” that claim simply doesn’t stand up to scrutiny.
Most of the study participants are members of one (or more) of four groups — the Jewish Therapist Collective, the Association of Jewish Psychologists, the Society of Pediatric Psychology Jewish Affinity Group, and Psychologists Against Antisemitism. Leaders of these groups have placed an emphasis on defending Israel, with a focus on defining and approaching antisemitism through that specific lens (the authors do not acknowledge this in their article). For example, one of these groups described APA’s leadership as “terribly naïve” for opposing the collective punishment of Palestinian civilians. Another has publicly accused the APA of “virulent” and “systemic” antisemitism based on members’ expressions of pain and outrage regarding Israel’s actions and concern for Palestinian lives. Two of the groups sponsor solidarity mission trips to Israel. To be clear, if the authors had wanted to do so, they presumably could have made a concerted effort to recruit participants from mental health organizations where Jewish members have a much wider range of perspectives on Israel and antisemitism (e.g., state psychological associations).
Meanwhile, those participants who were not recruited through these four groups were contacted via snowball sampling. With this form of outreach, researchers encourage potential recruits to share information about the study with their social network, to recruit them as well. The methodological problems associated with this approach are well-known. A snowball sample is rarely representative of the broader population of interest. As a result, research findings based on such a sample cannot legitimately be treated as generalizable beyond the specific profile of the self-selected group of participants. Given the overall process by which participants were recruited here, no reasonable claim can be made that their views and experiences — specifically regarding what does or doesn’t count as antisemitism — accurately characterize the much larger community of Jewish mental health professionals. To offer a parallel example, you can’t ask those individuals who attend a midnight showing of The Texas Chainsaw Massacre whether they like horror films and then conclude that their responses reflect the appeal of such films to moviegoers in general.
Further evidence of the authors’ highly biased sampling is available in their recruitment materials and in the introductory section of the online survey itself. The recruitment letter included this: “We are conducting a research study to understand the experiences of antisemitism among Jewish mental health professionals…We are particularly interested in any experiences of antisemitism people may have had in a professional or training context and how this has impacted career development and satisfaction.” Certainly, one would expect this description to draw particular interest from individuals who see themselves as having been victimized in this way, and much less interest from those who don’t.
The introduction to the survey gave this explanation for why the research was being conducted: “Since October 2023, a national increase in antisemitic incidents has been documented by several organizations, including the Anti-Defamation League and the Federal Bureau of Investigation. However, less is known about how antisemitism is manifesting in the mental health profession and how such manifestation may be impacting the functioning of Jewish professionals.” It’s hard to miss the suggestion that the “antisemitism” of primary interest to the researchers manifests in relation to Israel. Moreover, citing discredited data from the Anti-Defamation League — an Israel advocacy organization known to explicitly equate anti-Zionism with antisemitism and to count anti-genocide protests as antisemitic incidents — clearly communicates the researchers’ own perspective to prospective participants.
The bottom line is that the findings from this sample are not generalizable to the much broader and more diverse community of Jewish mental health professionals. In my opinion, the authors fail to adequately explain this crucial concern to readers.
Problematic Data Analyses
But beyond these very serious sampling problems, there’s also much about the study’s data analyses that call its value into question, and this too is worthy of attention. Here I’ll only focus on the two survey items that are the basis for the article’s highlighted figures and for the authors’ claims that antisemitism is widespread in mental health professionals’ work settings. The first of these two items looks approximately like this:
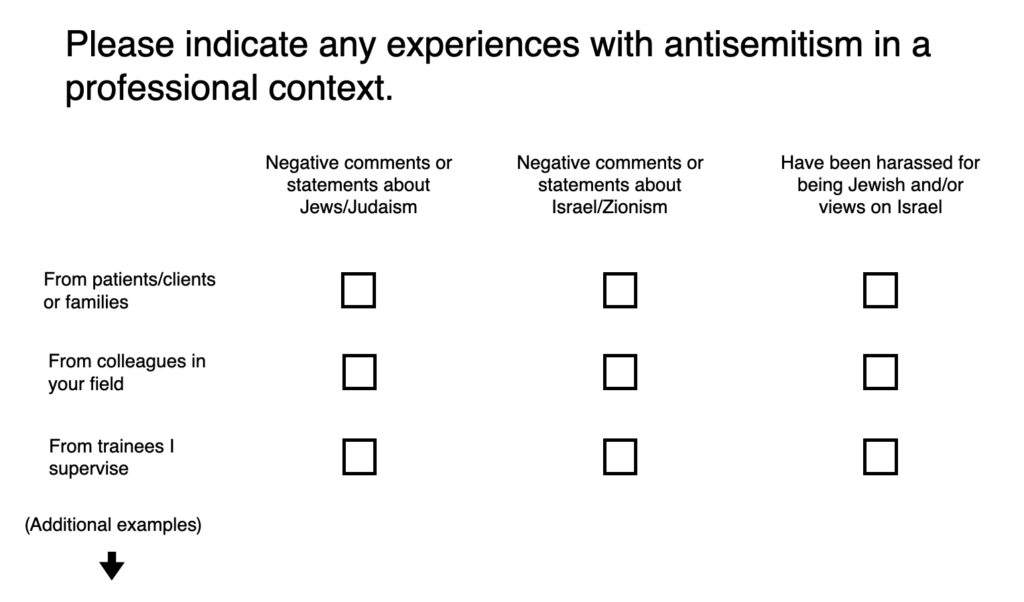
Respondents were asked to “Please indicate any experiences with antisemitism in a professional context” by checking a box if they’ve ever had that experience in eight different contexts (I’ve shown only the first three here). Three columns were provided: “Negative comments or statements about Jews/Judaism,” “Negative comments or statements about Israel/Zionism,” and “Have been harassed for being Jewish and/or views on Israel.” This framing and format are very problematic.
To begin with, the researchers explicitly presented negative comments about Israel or Zionism as a form of antisemitism (see the second column), and they made no distinction between “being Jewish” and “views on Israel” as the basis for “harassment,” a term that was never defined (see the third column). Obviously, the researchers’ framing of this item in regard to Israel reflects a view of antisemitism that is highly contentious, yet they take their own perspective as definitive. If they simply assumed that their participants would be comfortable with this framing, then that’s further evidence of the significant bias in their selection process. And if there were respondents who did not consider criticism of Israel to be antisemitic, these individuals may well have discontinued their participation when they learned that this was the researchers’ basic premise. Adding to the methodological confusion, in the article the authors acknowledge that many of their participants in fact didn’t tend to separate criticism of Israel or Zionism from hostility toward Jews. But what this seemingly means is that these respondents were likely to check boxes in two or even three columns at the same time for a single negative comment they heard about Israel.
This item suffers from other serious inadequacies as well. More specifically, the researchers made no attempt to assess the frequency with which participants were exposed to comments they deemed antisemitic, nor did they provide any timeframe to guide the respondents in their answers. So, for example, if a participant heard one colleague make one negative comment about Israel at any point — even if it was several months or years earlier — they were expected to check the box indicating that they had experienced antisemitism (actually, they could check all three columns if they felt that single comment was also hostile toward Jews and constituted “harassment”). The potential distortions here should be clear. Even more extreme cases are also plausible. For instance, if several dozen participants all read the same negative comment on a professional listserv, that one post would apparently be counted as an antisemitic experience for all of them simultaneously. In short, how useful could data like this possibly be for measuring the actual prevalence or severity of antisemitism in the work environment?
Beyond these significant issues, it’s worth highlighting that the researchers apparently gave no consideration to the legitimacy or appropriateness of any comment. Imagine a colleague saying, “It’s really upsetting to see that Israel is restricting the entry of humanitarian supplies into Gaza. I don’t understand why they’re doing that — it just seems terribly wrong to me.” Because that statement is certainly a “negative comment” about Israel, by the standards the authors established, hearing this would seemingly count as a harmful antisemitic experience. But how could such a comment, expressing concern and confusion, reasonably merit being categorized as antisemitic? And yet in this study it presumably would have been, at the researchers’ direction.
The second key survey question (the basis for Figure 2 in the article) asked, “In what ways, if any, has antisemitism appeared to impact career development or satisfaction?” Participants were asked to consider a range of categories and to check a box for each if, in their view, that experience with antisemitism applied to them. Recall that, at this point, the survey’s item wording had already communicated to the participants that criticism of Israel should be counted as antisemitic. The two categories with the highest endorsement rates were “Have triggered moments of heightened anxiety in professional settings” and “Have harmed personal and professional relationships with colleagues.”
For both categories, the researchers again failed to ask the respondents to identify the frequency or the timeframe associated with their adverse experiences. So, if a participant recalled a single day, perhaps months or years earlier, when they felt anxious following a colleague’s negative comment about Israel, that isolated event would still merit checking the box indicating that antisemitism had adversely affected the respondent’s professional life. Likewise, if that same single comment also diminished the respondent’s positive feelings toward this particular colleague, that too would count as a separate and additional affirmative case of having been harmed by antisemitism. Again, with this kind of coding, how could these items meaningfully illuminate the question of how serious a problem antisemitism is?
Other categories for this item represent different but similarly substantial interpretive problems. For example, consider these three separate categories: “Have been intentionally excluded from professional meetings/conferences or organizational activities,” “Have been unintentionally excluded from professional meetings/conferences or organizational activities,” and “Have been blocked or excluded from professional listservs or social media pages.” In each instance, an obvious question arises: how did the respondents know that antisemitism was the basis for these adverse experiences? But that question wasn’t asked. In some cases, participants may have received feedback that was clearly antisemitic in nature. Yet it seems unlikely that this was the norm. Conference proposal rejections, for instance, don’t routinely specify a reason. Moreover, whether right or wrong, if a participant was excluded based on their advocacy in support of Israel’s actions, that’s still not the same thing as being excluded for being Jewish — and only the latter is an unmistakable case of antisemitism. In short, lacking documentation, it’s quite a stretch for the authors to count all of these negative experiences as clear evidence of antisemitism. If the researchers instead recognize that these particular data merely reflect the participants perceptions of antisemitism, then that’s obviously not an adequate way to measure antisemitism’s actual prevalence.
I’ll dispense with other concerning aspects of the data analysis. Hopefully I’ve made my point. But I want to note that a much fuller explanation is needed for why the authors decided that “Out of concern for the sensitive nature of the data and participant confidentiality, raw data are not publicly available for this study.” In this regard, the survey protocol specifically stated that, through their participation, the respondents were agreeing to the sharing of their data. In fact, the online form emphasized that sharing data “is part of research and may increase what we can learn from this study” and that it “is needed to allow other researchers to validate study findings and to come up with new ideas.” Why then are the de-identified raw data being withheld? Without further clarity about this, from the perspective of pursuing science to advance our collective knowledge, I find this lack of transparency peculiar and inexplicable, and therefore quite troubling.
Concluding Observations
Given the skewed sample and how the authors chose to collect and analyze the survey data, their prediction that “there would be high levels of antisemitism reported by participants” is hardly surprising. And, of course, they treat their findings as confirming that prediction. But what did their results actually show? It seems to me that this is all the research demonstrated: if you cast your net very carefully, you can find some Jewish mental health professionals who at least once have felt somewhat uncomfortable in their work settings for reasons that they and the authors consider to be antisemitism. This is hardly noteworthy, regardless of the spin that may be applied by those who want to portray the mental health professions as overrun with antisemites.
To be clear, none of my commentary is meant to deny the discomfort and adversity reported by some participants in this study, or the fact that there’s complexity surrounding issues of antisemitism. Without question, there are very real instances of antisemitism in the mental health field — situations where someone is treated inappropriately because they’re Jewish. Some of the anecdotal accounts provided by participants clearly document this unfortunate reality. Such mistreatment is simply unacceptable, and it shouldn’t happen.
But to state the obvious, occupation, apartheid, war crimes, and genocide shouldn’t happen either, and criticizing Israel for these grave offenses shouldn’t be condemned as antisemitic. The Hamas-led attacks on October 7, 2023, were indisputably horrific and traumatizing. Yet certainly the same must be acknowledged about the 70,000 Palestinians killed by the Israel Defense Forces in Gaza (over twice that number have been injured) and the 2,000,000 permanently displaced from homes that were turned into rubble. (The word “Gaza” appears only twice in the article, and only in the context of the Israeli hostages.)
By an overwhelming margin just last month, the APA’s governing Council of Representatives adopted a new and clarifying resolution on antisemitism that’s relevant here. In particular, it highlights this point: “Multiple contemporary definitions of antisemitism all share the recognition that antisemitism involves hostility, prejudice, discrimination, harassment, hatred, or violence against Jews as Jews” (emphasis added). The resolution also notes that “the weaponization of antisemitism — the manipulative or bad faith invocation of accusations to silence legitimate criticism, scholarship, or activism — creates significant adverse consequences for Jews and non-Jews who oppose the state of Israel’s actions and support Palestinian rights.”
The authors conclude their article with three assertions that I consider both revealing and disturbing. First, they insist that “non-Jewish voices” should be given lesser status in any discussions about what does and doesn’t constitute antisemitism — this would presumably include discussions about criticism of Israel and support for Palestinian rights. Second, without evidence, they appear to claim that Jews who are not strong advocates for Israel — and do not see criticism of Israel as antisemitic — should be understood to hold “minority Jewish perspectives.” And third, they recommend that the Association of Jewish Psychologists — the organization mentioned earlier that criticized the APA’s opposition to the collective punishment of Palestinian civilians — should be awarded a seat on APA’s Council as an ethnic psychological association.
These convictions — especially given the article’s methodologically fragile findings —suggest to me the possibility that the broader research agenda of the authors (or at least some of them) is to advance a particular political framing of antisemitism, one that’s aimed above all else at protecting Israel from legitimate criticism. I believe such a project harms Jews and non-Jews alike, in our own professional circles and well beyond. Because while antisemitism is certainly a growing threat that deserves urgent attention from us all, protesting genocide and supporting Palestinian rights are not antisemitic. Antisemitism’s most powerful engines are very different: the ideologies of Christian nationalists and white supremacists, the Trump Administration, and Israeli leaders who falsely claim that Israel acts on behalf of all Jews worldwide.
To summarize my perspective, I think it’s deceptive and dangerous for the authors to claim that their results “indicate that antisemitism and the status of Jews and Jewishness within mental health fields are clearly widespread issues.” From the outset, their non-representative sample couldn’t possibly support such broad conclusions. And at this fraught moment, I believe we must not lose sight of the fact that sweeping and unwarranted claims of antisemitism have been used repeatedly to justify punitive governmental and institutional crackdowns on free speech and other democratic values.
I honestly cannot fathom why the editors and peer reviewers at the American Psychologist decided to publish this article given the shortcomings I’ve described. Regardless, my intention here has been to respectfully raise these significant red flags, and I hope I’ve accomplished that.
Roy Eidelson, PhD, is the past president of the Society for the Study of Peace, Conflict, and Violence (Division 48 of the American Psychological Association) and the author of Doing Harm: How the World’s Largest Psychological Association Lost Its Way in the War on Terror (McGill-Queens University Press, 2023).